Left Acetabular Roof Mri

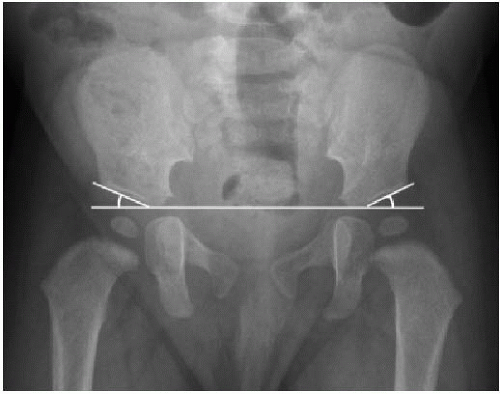
Acetabular Angle Radiology Reference Article Radiopaedia Org

This Radiograph Documents The Measurement Of The Acetabular Roof Download Scientific Diagram

Stress Fracture In Acetabular Roof Due To Motocross Case Report

Representative Example In Borderline Dysplastic Hip A Coronal Mri Download Scientific Diagram

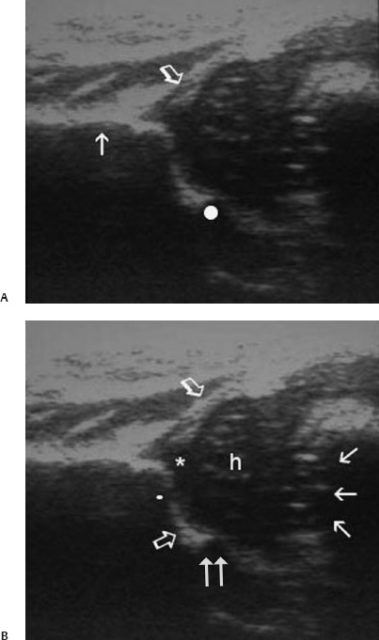
Mri Anatomy Of The Hip Review Mri Anatomy Of The Hip
Http Links Lww Com Jbjs E539
Surgical treatment involving resection of metastatic lesions and joint reconstruction using bone grafts is burdened with a high rate of complications.
Left acetabular roof mri.
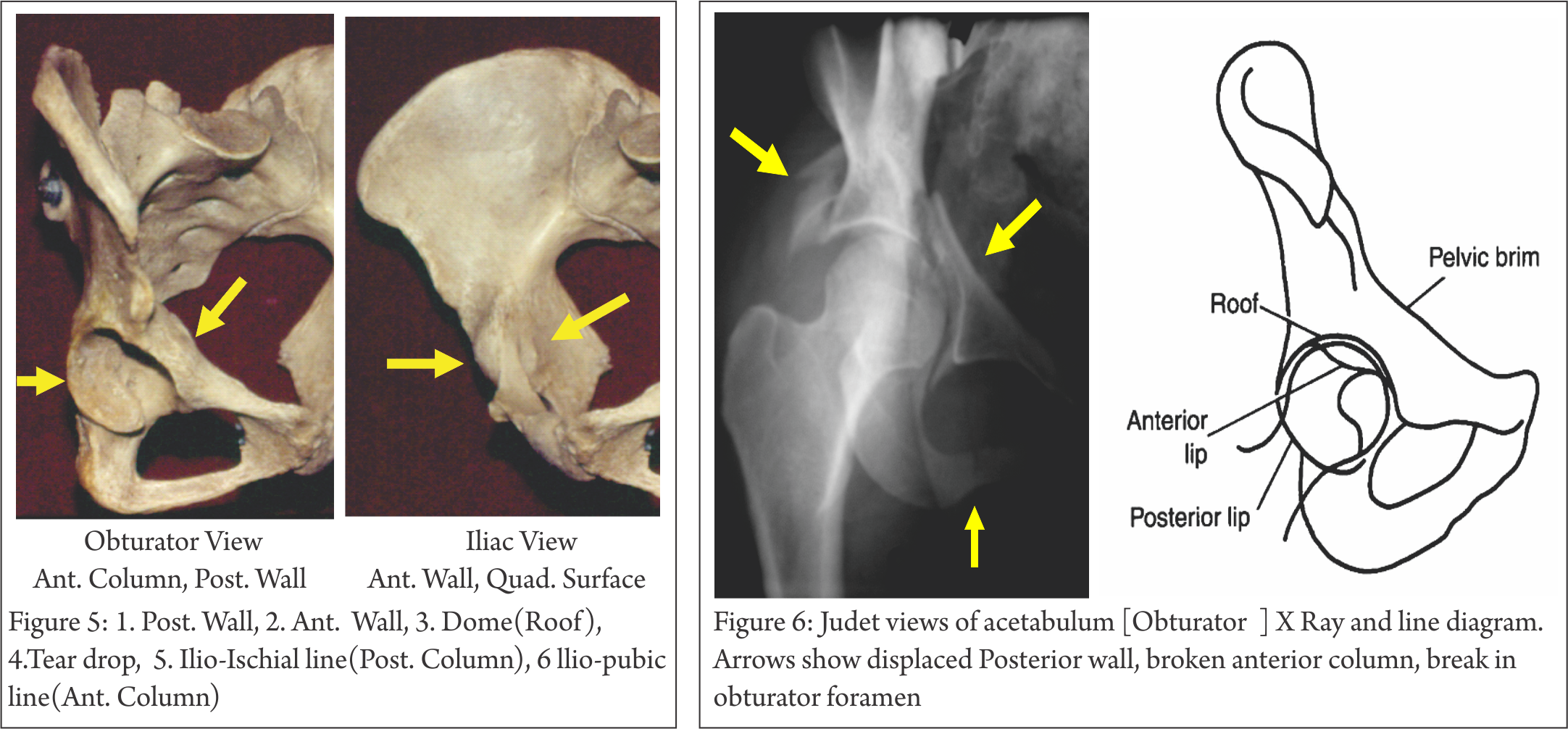
Understanding Clinical Radiology Of Fracture Acetabulum Trauma International

A Case Of Growth Disturbance Of The Acetabular Roof 5 3 Years Following Download Scientific Diagram

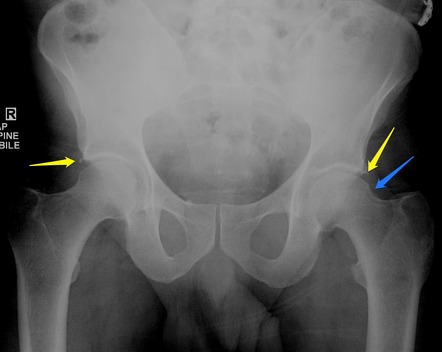
Developmental Dysplasia Of The Hip Radiology Reference Article Radiopaedia Org

Sketch Of The Three Main Types Of Acetabular Roof Dysmorphia A Download Scientific Diagram
Hip Disorders Radiology Key

Ct A And Mri T2w Fat Sat B At 2 Months After Surgery The Ct Scan Download Scientific Diagram

Measurement Of The Acetabular Index Ai From The Lateral End Of The Download Scientific Diagram
Os Acetabuli Radiology Reference Article Radiopaedia Org
Presentation1 Radiological Imaging Of Developmental Dysplasia Of The

Stress Fracture In Acetabular Roof Due To Motocross Case Report Sciencedirect

A Plain Radiograph Showing A Left Displaced Acetabular Anterior Wall Download Scientific Diagram

Imaging Of The Hip A Systematic Approach To The Young Adult Hip Abstract Europe Pmc

Girl With Left Hip Pain Mechanical Symptoms

A The Center Edge Angle Of Wiberg Dce Acetabular Roof Obliquity Download Scientific Diagram

Sclerotic Bone Leison Note Sclerotic Bone Leison In Tibia In Young Age Osteoid Osteoma Note Malignancy In Old Age Radiology Tumor Oral Pathology

Chapter 14 Pelvic Trauma Musculoskeletal Key

Radiographic Anatomy And Imaging Of The Acetabulum Sciencedirect
Http Pdf Posterng Netkey At Download Index Php Module Get Pdf By Id Poster Id 117296
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gctomex0gykvkjjeykmbpzcq5w25ug9wffu Trvyunwurzjyd4vm Usqp Cau

Pin By Contessa La Lobo On Peds Measuring Angles Radiology Ultrasound
Orif Through Modified Stoppa Approach For Anterior Column

Figure 2 From Desmoid Tumor Of Ilio Acetabular Region With Articular Cartilage Breach A Case Report Semantic Scholar

Pelvis And Perineum Radiology Key

Pelvic High Grade Chondrosarcoma Delayed Development Can Bisphosphonates Be Responsible A Case Report
Source : pinterest.com
